
Is TSH the only lab that matters—or should I be testing more?
TSH is not the only lab that matters for women with Hashimoto's thyroiditis—and in functional medicine, relying solely on it is one of the biggest oversights in conventional medicine. Many women feel persistently fatigued, brain-foggy, cold, or struggle with weight and mood issues despite "normal" TSH results. As I’ve said before functional medicine looks at the full picture: thyroid hormone production, conversion to T4 to T3, autoimmunity, nutrient status, inflammation, and root causes like gut health, stress, and toxins. It’s all about root cause health- the WHY.
Why TSH Alone Falls Short
TSH (Thyroid Stimulating Hormone) measures how hard your pituitary gland works to stimulate the thyroid. The pituitary sends thyroid stimulating hormone to the thyroid to tell it to make thyroxine or T4.
Conventional medicine uses it as usually the only marker, with "normal" ranges of 0.45–4.5 mIU/L. If TSH is high, doctors prescribe levothyroxine; if normal, they say you're fine. You know if your TSH is within the conventional lab ranges and they say you are fine but you don’t feel fine you are sent away. Women with thyroid problems are often written off as complainers, or they just need to exercise more, or you need an anti-depressant. I’m sure many of you know the drill. I’ve been there too.
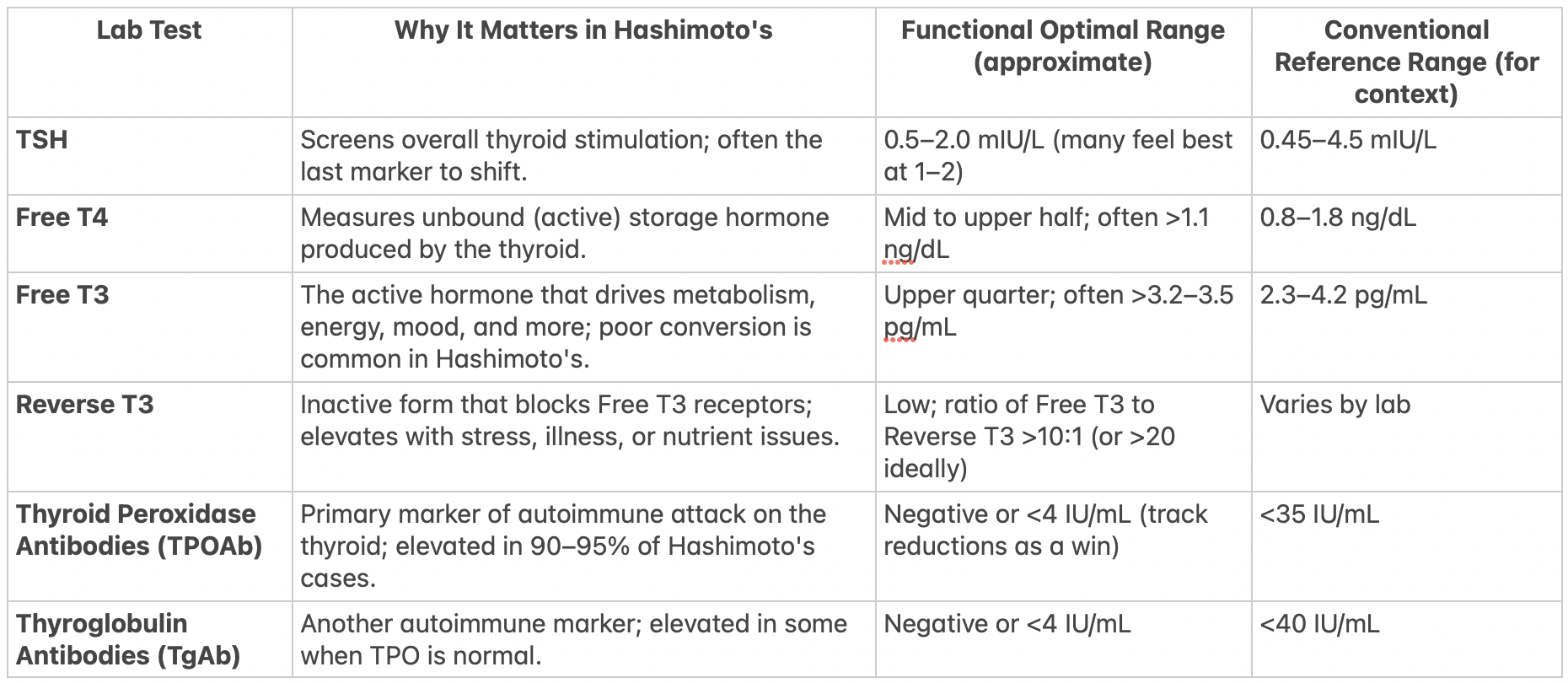
In functional medicine, relying solely on TSH is not the best marker to judge your thyroid function by because Hashimoto's thyroiditis is a progressive autoimmune condition where thyroid damage often begins long before TSH becomes abnormal. Even for someone who doesn’t have hashimoto’s and has just hypothyroidism, TSH is not the only or best marker to measure thyroid health. TSH plus Free T4 and Free T3 at a minimum should be measured by each and every doctor you see.
Hashimoto's involves the immune system producing antibodies (primarily TPOAb and TgAb) that attack thyroid tissue, leading to chronic inflammation and gradual destruction of thyroid follicular cells via cell-mediated and antibody-mediated mechanisms.
What exactly does this mean? This is the hard part- I’ve always been told that people don’t want to know the science. I was never like that even before I got my masters in nutrition. I wanted to know what was going on in my body because it helped me make informed decisions about my health, my diet, and my lifestyle. You can skip over this if you want but I feel like if you know what is going in in your body, it might help you understand why you feel the way you do.
Antibody mediated means that a type of white blood cell called a B cell makes TPO antibodies and thyroglobulin antibodies. The antibodies go around in your blood and bind to thyroid proteins. When they bind to those proteins it triggers damage to your thyroid gland in a couple of ways.
It activates a system in within your immune system called complement which is a group of proteins that poke holes in cell membranes, kind of like drilling into thyroid cells. They flag the cells for destruction - for other immune cells called natural killer cells to come in and kill the cells. This process keeps your thyroid from functioning by blocking thyroid peroxidase enzymes. These are the ones that that help T4 and T3 exist. This is why high antibody levels indicate you have hashimoto’s. These things are a sign of the attack and part of the weaponry of the autoimmune process.
Cell Mediated is about the immune attacks carried out by the immune cells themselves rather than the antibodies. It is kind of like hands on destruction. These immune cells, called T cells physically interact with and kill cells targeted for destruction. This is a major player in Hashimoto’s. These immune cells attack thyroid cells and the tissue within the thyroid gland becomes infiltrated with white blood cells out for destruction. This causes inflammation in the thyroid gland, scarring of tissue (this is when an ultrasound comes in handy).
These two processes work together to destroy your thyroid tissue which also can destroy your health, your joy, your energy, your everything. The attack happens gradually and progresses slowly- you can have significant damage before you have symptoms like fatigue, weight gain, etc become so obvious that you know something is wrong.
This process can unfold in stages:
Early stages: Genetic predisposition plus triggers like stress, infections, or toxins lead to elevated antibodies with normal TSH, Free T4, and Free T3—you may already feel symptoms like fatigue or brain fog.
Progressive inflammation: Thyroid becomes leaky or inefficient, but the pituitary gland still compensates by showing normal TSH output.
Later stages: As thyroid tissue is destroyed, hormone production drops, Free T4/T3 decline, and TSH finally rises (often considered "overt" hypothyroidism when TSH >10 mIU/L with low Free T4).
By the time TSH is elevated, significant thyroid damage (up to 90% loss of function in some cases) may have occurred. Functional medicine emphasizes catching and addressing the autoimmune process early, when interventions can potentially slow or halt progression, rather than waiting for TSH to flag overt disease.
Why TSH Doesn't Reveal T4 to T3 Conversion Issues
The thyroid produces mostly T4 (about 93%), an inactive "storage" hormone that must be converted peripherally (mainly in the liver, gut, and kidneys) to active T3 via enzymes called deiodinases. This conversion is crucial because T3 is what binds to receptors and drives metabolism, energy, mood, and virtually every cell function.
In Hashimoto's (and hypothyroidism generally), conversion is often impaired due to:
Inflammation inhibiting deiodinase activity.
Nutrient deficiencies.
Stress or illness shifting conversion toward inactive Reverse T3.
TSH only reflects pituitary signaling based on circulating T4/T3 levels—it doesn't measure how effectively T4 is activated to T3 or if T3 is reaching tissues.
Many women with Hashimoto's have "normal" TSH and Free T4 but low Free T3, leading to persistent hypothyroid symptoms despite treatment. Studies show selenium and zinc are essential cofactors for deiodinases; deficiencies reduce T4-to-T3 conversion, and supplementation can improve it
What High Reverse T3 Means
Reverse T3 (rT3) is an inactive molecule of T3 produced from T4 under stress, inflammation, illness, fasting, or nutrient deficits. It binds to T3 receptors but does nothing—essentially blocking active T3 from working, like putting the wrong key in a lock. This is an adaptive "energy conservation" mode (seen in "non-thyroidal illness syndrome" or "euthyroid sick syndrome").
Elevated rT3 is common in chronic stress, infections, or inflammation—prevalent in Hashimoto's. TSH remains normal because total hormone levels aren't critically low, but cellular thyroid action is impaired, causing hypothyroid-like symptoms. Functional medicine tests rT3 and the Free T3:rT3 ratio (>10–20 ideally) to uncover this hidden issue.
Thyroid Ultrasound: What It Entails and Why It's Recommended
A thyroid ultrasound can visualize the gland's size, texture, blood flow, and any nodules. In Hashimoto's, classic findings include:
Diffuse enlargement (goiter) or atrophy.
Uneven or patchy looking thyroid tissue due to infiltration of white blood cells damaging tissue.
Increased vascularity (inflammation).
Pseudonodules (lumpy appearance from inflammation, not true nodules).
It's recommended at least once (or if symptoms/neck issues) because it confirms autoimmune inflammation even when labs are borderline, rules out nodules/cancer risk, and tracks progression. I’ve never had any practitioner or doctor recommend an ultrasound. I do think it is a good idea.
Why Total T3/T4 Are Less Useful Than Free T3/4
Most thyroid hormones circulate bound to proteins (e.g., TBG). Total T3/T4 measure bound + unbound, while Free T3/T4 measure only the unbound, biologically active fraction available to tissues.
Total T4/T3 can fluctuate misleadingly due to pregnancy, estrogen (birth control), liver issues, or inflammation altering binding proteins—without reflecting true thyroid status. Free levels are more reliable for assessing function, especially in complex cases like Hashimoto's.
Nutrient Deficiencies Critical for Thyroid Function and Immunity
Hashimoto's increases nutrient needs while impairing absorption (due to inflammation/gut issues). Key ones:
Selenium — Supports T4-to-T3 conversion, reduces oxidative stress, and lowers TPO antibodies. Multiple RCTs show 200 mcg/day reduces antibodies by 20–50% in 6–12 months.
Vitamin D — Modulates immunity; low levels correlate with higher antibodies and autoimmunity risk. Supplementation often improves outcomes.
Ferritin (iron storage) — Needed for thyroid peroxidase enzyme (makes hormones). Low ferritin (<70–90 ng/mL) common, causes hair loss/fatigue independent of anemia.
Vitamin B12 — Up to 40% deficient; causes fatigue, neuropathy mimicking hypothyroidism.
Others: Zinc (conversion), iron (synthesis).
Adrenals, Stress, and Blood Sugar in Hashimoto's
Chronic stress is a well-documented trigger for Hashimoto's onset/flares via HPA axis dysregulation, immune shifts toward Th1/Th17 responses, and increased inflammation/oxidative stress. The exact "90%" figure for adrenal dysfunction appears more in clinical cases rather than large peer-reviewed studies—research shows frequent HPA alterations but variable prevalence.
In chronic stress, cortisol patterns (via 4-point saliva/urine) often show:
Early: High overall cortisol.
Prolonged: Flattened curve—low morning (no wake-up surge), high evening (trouble sleeping), or overall low ("adrenal fatigue" pattern).
Blood sugar instability ties to adrenals because cortisol/glucagon raise glucose during stress; unstable sugar (highs/crashes from poor diet) repeatedly activates adrenals, worsening HPA fatigue. This exacerbates both adrenal (anxiety, crashes) and thyroid symptoms (fatigue, conversion blocks via high rT3) by increasing inflammation.
Leaky Gut, Infections, and Molecular Mimicry
Leaky gut (increased intestinal permeability) allows undigested food particles, bacteria, or toxins into bloodstream, triggering systemic immune activation.
In Hashimoto's, this can initiate/maintain autoimmunity via molecular mimicry—where foreign proteins (e.g., gluten's gliadin, bacterial peptides from Yersinia/EBV/H. pylori) structurally resemble thyroid tissue (e.g., thyroglobulin or peroxidase).
The immune attack on the mimic cross-reacts with thyroid, perpetuating antibodies/inflammation.
How General Inflammation Affects Thyroid Health
Chronic low-grade inflammation (from diet, stress, gut issues) promotes autoimmunity by activating immune cells, increasing cytokines that damage thyroid tissue and impair hormone synthesis/conversion.
High-sensitivity C-reactive protein (hs-CRP) and erythrocyte sedimentation rate (ESR) are two common blood tests used to detect and monitor systemic inflammation in the body. They're non-specific—meaning they don't pinpoint the exact source of inflammation—but they're valuable for assessing overall inflammatory status.
hs-CRP: This is a protein produced by the liver in response to inflammatory signals, primarily interleukin-6 (IL-6) and other cytokines released during immune activation. The "high-sensitivity" version detects very low levels of inflammation (below 10 mg/L), making it useful for chronic, low-grade issues rather than acute infections. Levels are categorized roughly as:
Low risk: <1 mg/L
Average: 1–3 mg/L
High: >3 mg/L (with >10 mg/L often indicating acute inflammation)
In functional medicine, hs-CRP is favored because it's more sensitive and responsive to subtle changes.
ESR: This older test measures how quickly red blood cells (erythrocytes) settle at the bottom of a test tube over an hour (reported in mm/hr). Inflammation causes proteins like fibrinogen to clump red cells together, making them settle faster. Normal ranges are roughly 0–20 mm/hr for women (higher with age). It's less specific and can be influenced by anemia, pregnancy, or other factors.
Both rise in response to inflammation from infections, autoimmunity, injury, obesity, or chronic conditions—but hs-CRP tends to rise and fall more quickly, while ESR is slower.
Their Role in Thyroid Dysfunction, Especially Hashimoto's
In Hashimoto's thyroiditis and hypothyroidism, there's often a bidirectional relationship with inflammation: The autoimmune process creates inflammation, which damages the thyroid, and thyroid dysfunction can itself promote systemic inflammation (e.g., through altered lipid metabolism or oxidative stress).
Elevated hs-CRP in Hashimoto's/Hypothyroidism:
Multiple studies show that patients with autoimmune hypothyroidism (including Hashimoto's) have significantly higher hs-CRP levels compared to healthy controls, even in subclinical cases. This reflects low-grade systemic inflammation driven by the autoimmune attack (cytokines like IL-6 and TNF-α stimulating CRP production). Higher hs-CRP is also linked to increased cardiovascular risk in these patients, as inflammation promotes atherosclerosis.
Interestingly, treating with levothyroxine often lowers hs-CRP, suggesting that restoring thyroid function reduces inflammation. However, if hs-CRP remains high despite "normal" TSH, it may point to ongoing root causes like gut issues or other inflammatory triggers.ESR in Hashimoto's/Hypothyroidism:
ESR is typically normal or only mildly elevated in chronic Hashimoto's, unlike in painful subacute thyroiditis (where it's often markedly high, >50–100 mm/hr). Some studies show slight elevations in hypothyroid groups overall, but it's not as reliable or sensitive as hs-CRP for monitoring Hashimoto’s.
How Systemic Inflammation Impacts Thyroid Function
Inflammation doesn't just reflect thyroid problems—it actively worsens them through several mechanisms:
Impaired Hormone Conversion: Inflammatory cytokines (e.g., IL-6, TNF-α) inhibit deiodinase enzymes, reducing conversion of T4 to active T3 and increasing inactive Reverse T3. This contributes to persistent symptoms despite treatment.
Perpetuating Autoimmunity: Chronic inflammation (from any source—gut dysbiosis, food sensitivities, stress) upregulates immune responses, potentially increasing antibody production (TPOAb/TgAb) and thyroid tissue damage.
Direct Thyroid Effects: Severe inflammation can temporarily suppress TSH or cause "non-thyroidal illness syndrome," but in autoimmune cases, it sustains the cycle of destruction.
From a functional medicine perspective, elevated hs-CRP (even mildly, like 1–3 mg/L) or ESR signals broader inflammatory burdens that could be fueling Hashimoto's flares or preventing remission.
Practitioners use these to guide interventions: anti-inflammatory diets (e.g., removing gluten/dairy), gut healing, or addressing infections/toxins. Lowering inflammation often correlates with better thyroid function, reduced antibodies, and improved symptoms.
These markers aren't diagnostic for Hashimoto's alone (antibodies and thyroid hormones are key), but tracking them provides insight into progress beyond TSH. Always interpret in context—work with a practitioner, as levels can fluctuate.
Toxins and Thyroid/Autoimmunity
Environmental toxins act as endocrine disruptors:
Heavy metals (mercury, lead) compete with minerals, increase oxidative stress.
BPA/plastics, pesticides interfere with hormone binding/receptors.
Mold mycotoxins suppress immunity and trigger inflammation.
These can mimic/trigger autoimmunity or directly impair thyroid function.